






Age-related cognitive impairment has become a global public health problem with the rapid population aging worldwide. Cognitive impairment causes function loss and dependency for those suffering from the disorders, poses a significant burden to their family [ 1 ], and brings tremendous challenges to the health care system and society [ 2 ]. Delving into novel approaches that could promote healthy brain aging with higher accessibility is crucial to address this problem, which is especially true to low- and middle-income countries, where a large number of residents are suffering from cognitive impairment but professional resources are limited [ 3 ].
In recent years, social participation (SP) has been regarded as a potentially effective approach considering its wide accessibility as well as its theoretical effect on cognitive function [ 4 ]. Prior studies have proposed three plausible mechanisms between SP and cognitive function. First, the ‘use it or lose it’ hypothesis suggests that participating in social activities may increase one’s cognitive activities that contribute to more mental stimulation and better brain function [ 5 ]. Second, the increased physical activities derived from taking part in social activities may help sustain cerebral blood flow, increase aerobic capacity and cerebral nutrient supply, thus lower the risk of cognitive impairment [ 6 ]. Third, SP may help one increase interpersonal interaction, obtain more social support, reduce the risk of suffering from psychological stress, and mitigate the stress-related neuronal changes that lead to cognitive decline [ 7 ].
Despite the broad agreement on the general benefit of SP on cognitive function [ 8 ], several knowledge gaps remain. First, since SP is an umbrella term that covers a broad range of activities, the relationship between a specific type of SP and cognitive function has not reached an agreement. For instance, a statistically significant association was observed between cognitive function and voluntary activities and interaction with friends in some studies [ 9 , 10 ] but not in others [ 11 , 12 ]. The underlying reason may be that the social significance of SP varies across cultural contexts [ 13 ], which calls for further investigation from an embeddedness perspective. Second, prior literature indicates that different types of SP translate to improved cognitive function through different paths [ 14 ]. For instance, internet use may contribute to better cognitive function through improved memory in information searching and processing [ 15 ]. Meanwhile, visiting friends involves increased social interactions [ 16 ]. The associated social support has been suggested to benefit both memory and executive functioning through reduced depressive symptoms [ 17 ]. However, the majority of the extant epidemiological studies treated cognitive function as a whole using scales such as Mini-Mental State Examination (MMSE) [ 11 , 18 ], leaving how the association holds across different dimensions of cognitive function in practice largely understudied. Such differences are critical for the development of targeted interventions. Third, most of the published studies only concerned observable variables, with unmeasurable individual-level confounding factors not controlled. Individual-level characteristics, such as gene, intelligence, and personality, may influence one’s health behaviours and mental health simultaneously [ 19 , 20 ]. Not considering the individual heterogeneity may lead to overestimation of the association or spurious correlation. Moreover, the vast majority of the limited evidence was from western countries, leaving what is happening in Chinese culture mostly unknown.
Under such circumstances, the present study has two aims: 1) to understand the patterns of SP and cognitive function in China’s context across a four-year period; 2) to explore the relationship between SP and cognitive function by digging down to specific types of SP and two dimensions of cognitive function. We hypothesised that: 1) in general, more types and higher frequency of SP is associated with improved cognitive function; and 2) the magnitude of association varies across different types of SP and different dimensions of cognitive function. We employed a fixed-effects analysis to address biases from omitted time-invariant variables. In light of the evident gender difference in China that strongly influences the SP behaviours and cognitive function in various ways [ 21 ], we further tested the association in subgroups.
Sample and data collection
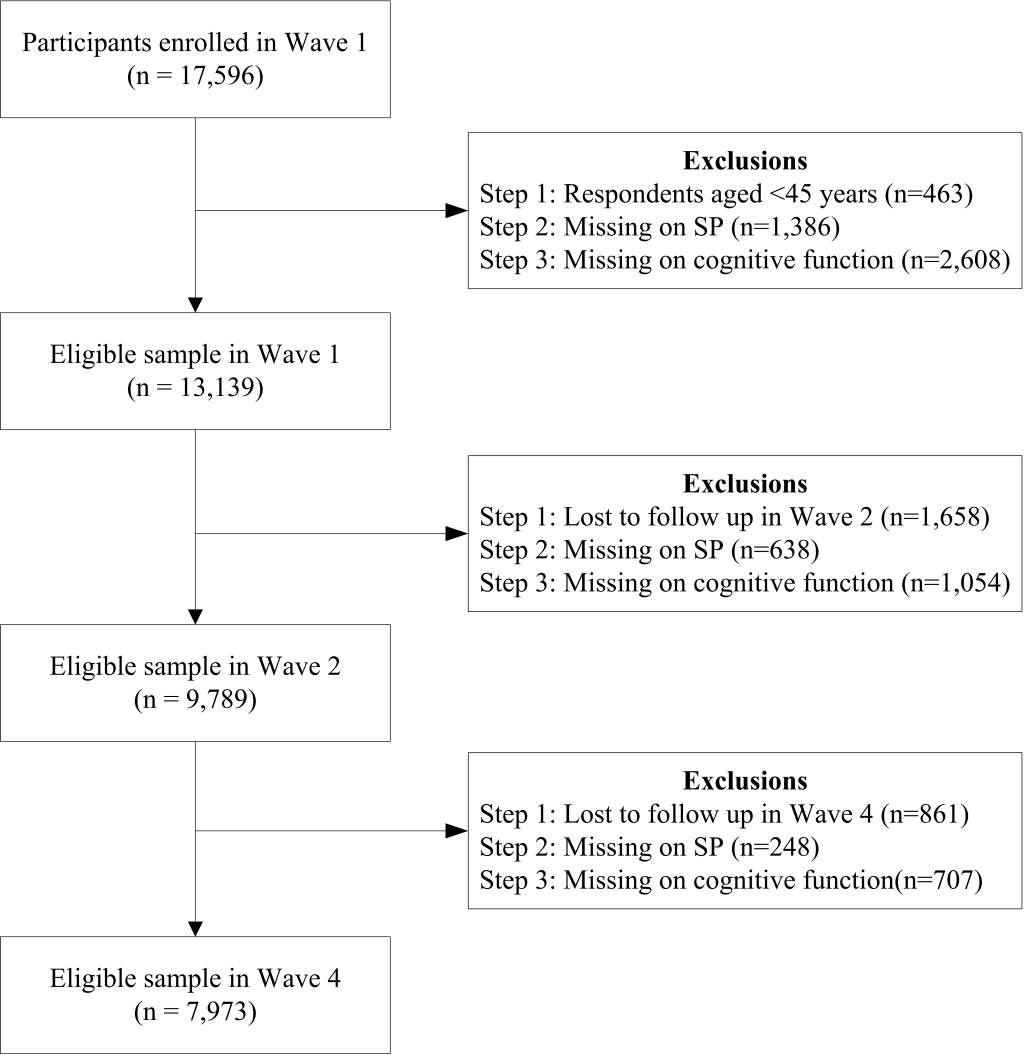
The data set used for statistical analysis in this study came from the China Health and Retirement Longitudinal Study (CHARLS). Underpinned by the multistage stratified probability proportional to size (PPS) sampling technique, the CHARLS research team surveys middle- and old-aged community-dwelling residents from 450 villages in 150 counties of 28 provinces in China. The baseline study was carried out in 2011 and involved 17 596 residents. Biannual follow-ups were conducted in 2013 and 2015. Considering that the fixed-effects regression examines the relationship between changes in independent and dependent variables across all three waves, a total of 7973 respondents were selected according to the selection process ( Figure 1 ). We also implemented multiple imputation for missing data amongst those who participated in all three waves to check the robustness of our results, which yielded similar results (Table S1 in the Online Supplementary Document ).
Variables
Cognitive function
Similar to the US Health and Retirement Study, CHARLS employed components of the Telephone Interview of Cognitive Status (TICS) battery. Prior studies suggested measuring one’s cognitive function from two dimensions, including memory and a second factor labelled as ‘mental status’ [ 21 , 22 ]. Memory was measured by testing one’s skills relating to immediate word recall (0-10 points) and delayed word recall (0-10 points). Mental status was measured from three aspects, including orientation, visuoconstruction, and mathematical performance. Orientation (0-5 points) was measured by asking respondents to name today’s date, day of the week, and season; visuoconstruction was assessed by re-drawing a previously shown picture (0-1 point); mathematical performance (0-5 points) was measured by subtracting 7 from 100 consecutively for five times. We constructed the cognitive function from these two components (0-31 points) with higher scores suggesting better cognitive function.
Social Participation
We extracted seven types of SP from CHARLS, including 1) interaction with friends, 2) playing mah-jong or other board games, 3) going to sports or social clubs, 4) joining community-related organisations, 5) undertaking voluntary activities; 6) providing help to relatives or others without compensation, and 7) Internet use. For each type of SP, CHARLS [ 23 ] asked the respondent whether they had taken any of the aforementioned SP in the last month. If yes, they were further asked about the frequency accordingly (almost daily/ almost every week/ not regularly).
In this study, we examined SP from three aspects, namely type, maximum frequency, and diversity.
Type: since the proportion of those who took daily SP was less than 0.5%, we merged the two clusters ‘almost daily’ and ‘almost every week’ and recoded as ‘≥1/week’ for each type of SP. For the two variables ‘undertaking voluntary or charity activities’ and ‘providing help to relatives or others without compensation’, considering the small proportion of those who took these types of SP (less than 2%), we merged them to construct a new variable ‘voluntary activity’, following Lin’s [ 24 ] study. For ‘sports or social clubs’, ‘community organisations’, and ‘Internet use’, the proportion of the respondents with a frequency of once a week or higher was less than 1%. We then dichotomised them into No/Yes. Maximum frequency : the highest frequency of the aforementioned six types of SP, and was coded as: No/ not regularly/≥1/week. Diversity : we summed up the total number of types of SP and categorised it into: None/ 1 type/≥2 types.
Covariates
The confounding variables came from three aspects, including socio-demographic characteristics, health behaviours, health status-related variables, and time variable. For socio-demographic characteristics, we included gender, age, residency (rural, urban), education (illiterate, primary school and lower, junior middle school, senior middle school and higher), retirement (no, yes), marital status (single, partnered), living near children (no, yes), and percapital household income (Total household income (in US$)/ number of people in the household). For health behaviours, we considered current alcohol consumption (no, yes), and current smoking (no, yes). With respect to health status-related variables, we included numbers of types of non-communicable diseases (none, 1 type, 2 types, ≥3 types), and numbers of types of lower body constraints (none, 1 type, 2 types, ≥3 types). This study treated gender and residency as time-invariant variables, and the rest as time-varying variables.
Data analysis
The overall aim of this study was to assess the association between SP and cognitive function with personal level time-invariant endogeneity addressed. We performed descriptive and multivariate analyses. First, frequencies and percentages were calculated for categorical data, whereas mean value and standard deviation (SD) were computed to describe normally-distributed continuous variables. χ 2 test and t test were performed accordingly. Second, we employed correlation analysis and cross-sectional regression analysis to describe the relationship between SP and cognitive function. To test the correlation between SP and cognitive function, we conducted Spearman test for ordinal variables such as interacting with friends, mah-jong, and voluntary activities, whereas t test was employed for binomial variables such as sports, internet use, and community organisations. For the cross-sectional regression, we used pooled data from 2011, 2013, and 2015, and controlled for all time-varying and time-invariant variables. The results from both correlation and cross-sectional regression analysis indicated that the positive association holds across different types of SP and different dimensions of cognitive function (Table S2 in the Online Supplementary Document ). Based on the results from the second stage analysis, we used a longitudinal linear fixed-effects regression model for further analysis. This model treats each individual as their own control and investigates how dependent variable changes as the independent variable changes. This, therefore, controls the potential individual-level time-invariant confounders, such as gene and personality, and helps us obtain reliable estimations regarding the relationship between SP and cognitive function.
Cognitive function it = μ t +β 1 SP it +β 2 x it +α i +ϵ it
Congitive function it indicates the cognitive performance for individual i at time t. SP it suggests the diversity, frequency, and type of SP for individual i at time t. x it denotes time-varying variables, such as health behaviours and health outcome variables. μ t captures year-specific effects, whereas α i characterises all time-invariant variables, such as gene and personality.
F-test and Hausman test were employed for model selection among ordinary least squares (OLS), random-effects model, and fixed-effects model. With a statistical significance ( P < 0.001) for both tests, the results indicated that OLS or random-effects model would be biased, whereas the fixed effects model was preferred.
Prior studies have revealed that SP brings immediate influence to one’s mental health, which may fade away as time passes by [ 20 ]. In light of a two-year interval between two CHARLS follow-ups, we assessed the contemporaneous association between changes in SP and that in cognitive function. Coefficients (β) with 95% Confidence Intervals (95% CIs) were employed to measure the effect. Data were analysed using R Version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Basic characteristics of the respondents
Table 1 presents the basic characteristics of the respondents in 2011. Amongst the 7973 respondents, a greater proportion were men, rural residents, with primary school or lower education, living with a partner and near children, and currently working.
| Characteristics | All (n = 7973) | Men (n = 4156) | Women (n = 3817) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Residency: | ||||||
| Urban | 3065 | 38.44 | 1502 | 36.14 | 1563 | 40.95 |
| Rural | 4908 | 61.56 | 2654 | 63.86 | 2254 | 59.05 |
| Age: | ||||||
| Mean (SD) | 57.79 (8.52) | 58.7 (8.58) | 56.8 (8.34) | |||
| Education: | ||||||
| Illiterate | 1442 | 18.09 | 347 | 8.35 | 1095 | 28.69 |
| ≤Primary school | 3474 | 43.58 | 1895 | 45.61 | 1579 | 41.37 |
| Middle school | 1969 | 24.70 | 1190 | 28.64 | 779 | 20.41 |
| ≥High school | 1087 | 13.64 | 723 | 17.40 | 364 | 9.54 |
| Per capita household income: | ||||||
| Median (1 st quartile, 3 rd quartile) | 805 (245, 1753) | 754 (228, 1690) | 857 (259, 1821) | |||
| Marital status: | ||||||
| Single | 742 | 9.31 | 304 | 7.31 | 438 | 11.47 |
| Partnered | 7231 | 90.69 | 3852 | 92.69 | 3379 | 88.53 |
| Living near children: | ||||||
| No | 642 | 8.24 | 376 | 9.33 | 266 | 7.07 |
| Yes | 7151 | 91.76 | 3656 | 90.67 | 3495 | 92.93 |
| Retirement: | ||||||
| No | 6030 | 75.85 | 3336 | 80.56 | 2694 | 70.73 |
| Yes | 1920 | 24.15 | 805 | 19.44 | 1115 | 29.27 |
| Alcohol consumption: | ||||||
| No | 5127 | 64.30 | 1756 | 42.25 | 3371 | 88.32 |
| Yes | 2846 | 35.70 | 2400 | 57.75 | 446 | 11.68 |
| Smoking: | ||||||
| No | 5338 | 66.95 | 1742 | 41.92 | 3596 | 94.21 |
| Yes | 2635 | 33.05 | 2414 | 58.08 | 221 | 5.79 |
| Types of NCDs: | ||||||
| No NCD | 2379 | 30.95 | 1336 | 33.27 | 1043 | 28.41 |
| 1 type | 2203 | 28.66 | 1166 | 29.03 | 1037 | 28.25 |
| 2 types | 1589 | 20.67 | 799 | 19.90 | 790 | 21.52 |
| ≥3 types | 1516 | 19.72 | 715 | 17.80 | 801 | 21.82 |
| Lower body constraints: | ||||||
| No constraint | 4112 | 51.57 | 2459 | 59.17 | 1653 | 43.31 |
| 1 type | 1692 | 21.22 | 817 | 19.66 | 875 | 22.92 |
| 2 types | 1117 | 14.01 | 466 | 11.21 | 651 | 17.06 |
| ≥3 types | 1052 | 13.19 | 414 | 9.96 | 638 | 16.71 |
Patterns of social participation and cognitive function
Table 2 depicts SP and cognitive function of the respondents in all three waves. Nearly half of the respondents did not take any social activities in all three waves, especially in voluntary activities, sports or social clubs, Internet or community organisations. However, an upward trend of conducting social activities was observed in these four types of SP, and so as the diversity of SP. Cognitive function generally declined after four years. Nevertheless, there was an improvement in memory during 2011-2013. In general, women were less likely to participate in SP and were more disadvantaged in cognitive function than their counterparts in all three waves.
| 2011 | 2013 | 2015 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Men | Women | All | Men | Women | All | Men | Women | |
| Social participation, % | |||||||||
| Diversity: | |||||||||
| None | 47.99 | 47.81 | 48.18 | 40.44 | 40.16 | 40.74 | 46.68 | 46.27 | 47.13 |
| 1 type | 33.12 | 31.98 | 34.37 | 34.48 | 33.83 | 35.18 | 28.67 | 28.18 | 29.21 |
| ≥2 types | 18.89 | 20.21 | 17.45 | 25.08 | 26.01 | 24.08 | 24.65 | 25.55 | 23.66 |
| Frequency: | |||||||||
| None | 47.99 | 47.81 | 48.18 | 40.44 | 40.16 | 40.74 | 46.68 | 46.27 | 47.13 |
| Not regularly | 14.76 | 15.66 | 13.78 | 16.71 | 18.14 | 15.14 | 16.33 | 17.81 | 14.72 |
| ≥1/week | 37.25 | 36.53 | 38.04 | 42.86 | 41.70 | 44.12 | 36.99 | 35.92 | 38.15 |
| Interacting with friends: | |||||||||
| None | 63.68 | 65.76 | 61.41 | 58.20 | 60.76 | 55.41 | 63.90 | 64.89 | 62.82 |
| Not regularly | 10.67 | 10.76 | 10.58 | 13.71 | 13.76 | 13.65 | 13.24 | 13.81 | 12.63 |
| ≥1/week | 25.65 | 23.48 | 28.01 | 28.09 | 25.48 | 30.94 | 22.85 | 21.29 | 24.55 |
| Mah-jong, cards, chess or other clubs: | |||||||||
| None | 78.65 | 74.76 | 82.89 | 76.50 | 71.78 | 81.63 | 78.74 | 74.88 | 82.94 |
| Not regularly | 9.01 | 10.71 | 7.15 | 8.98 | 11.21 | 6.55 | 8.42 | 10.25 | 6.42 |
| ≥1/week | 12.34 | 14.53 | 9.96 | 14.52 | 17.01 | 11.82 | 12.84 | 14.87 | 10.64 |
| Voluntary activities: | |||||||||
| None | 91.36 | 90.64 | 92.14 | 84.87 | 84.53 | 85.25 | 83.46 | 82.24 | 84.78 |
| Not regularly | 6.18 | 6.81 | 5.50 | 10.81 | 11.45 | 10.11 | 12.32 | 13.19 | 11.37 |
| ≥1/week | 2.46 | 2.55 | 2.36 | 4.31 | 4.02 | 4.64 | 4.23 | 4.57 | 3.85 |
| Sports or social clubs: | |||||||||
| No | 93.67 | 94.18 | 93.11 | 90.81 | 92.81 | 88.63 | 91.37 | 94.20 | 88.29 |
| Yes | 6.33 | 5.82 | 6.89 | 9.19 | 7.19 | 11.37 | 8.63 | 5.80 | 11.71 |
| Internet: | |||||||||
| No | 97.88 | 97.62 | 98.17 | 96.61 | 96.15 | 97.12 | 96.04 | 95.48 | 96.65 |
| Yes | 2.12 | 2.38 | 1.83 | 3.39 | 3.85 | 2.88 | 3.96 | 4.52 | 3.35 |
| Community organizations: | |||||||||
| No | 98.39 | 98.27 | 98.53 | 97.57 | 97.43 | 97.72 | 97.25 | 96.82 | 97.72 |
| Yes | 1.61 | 1.73 | 1.47 | 2.43 | 2.57 | 2.28 | 2.75 | 3.18 | 2.28 |
| Cognition, mean (SD) | |||||||||
| Total score | 15.41 (4.87) | 15.99 (4.54) | 14.78 (5.13) | 15.32 (5.11) | 15.91 (4.68) | 14.68 (5.49) | 14.59 (5.26) | 15.02 (4.91) | 14.12 (5.59) |
| Memory | 7.49 (3.26) | 7.48 (3.17) | 7.49 (3.35) | 7.55 (3.40) | 7.56 (3.27) | 7.53 (3.54) | 7.00 (3.52) | 6.89 (3.41) | 7.14 (3.62) |
| Mental status | 7.93 (2.71) | 8.51 (2.43) | 7.29 (2.86) | 7.78 (2.78) | 8.34 (2.50) | 7.16 (2.94) | 7.58 (2.80) | 8.13 (2.53) | 6.99 (2.97) |
SD – standard deviation
Association between SP and cognitive function
The associations between changes in SP and that in the total cognitive function, memory, and mental status across three waves are presented in Table 3 . Transmitting from no SP to more varieties or a higher frequency of SP was strongly associated with an improved cognitive function. The general association held across dimensions of cognitive function and gender subgroups. With the exception of joining community organisations, taking part in the other five types of SP was positively associated with a better cognitive function, amongst which, the association was most prominent for playing mah-jong.
| Total score | Memory | Mental status | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Men | Women | All | Men | Women | All | Men | Women | |
| β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | |
| Variety (Ref: None) | |||||||||
| 1 type | 0.377*** (0.192, 0.562) | 0.355* (0.080, 0.629) | 0.404** (0.154, 0.654) | 0.248*** (0.104, 0.391) | 0.208+ (-0.003, 0.419) | 0.291** (0.096, 0.487) | 0.129* (0.026, 0.233) | 0.147+ (-0.007, 0.300) | 0.113 (-0.028, 0.254) |
| ≥2 types | 0.703*** (0.470, 0.937) | 0.522** (0.178, 0.865) | 0.856*** (0.537, 1.175) | 0.440*** (0.258, 0.622) | 0.321* (0.056, 0.586) | 0.541*** (0.292, 0.791) | 0.263*** (0.130, 0.395) | 0.201* (0.008, 0.394) | 0.315*** (0.135, 0.494) |
| Frequency (Ref: None) | |||||||||
| Not regularly | 0.235* (0.007, 0.462) | 0.075 (-0.254, 0.405) | 0.378* (0.062, 0.693) | 0.119 (-0.058, 0.296) | -0.030 (-0.284, 0.223) | 0.260* (0.014, 0.507) | 0.115+ (-0.013, 0.243) | 0.106 (-0.079, 0.290) | 0.117 (-0.060, 0.295) |
| ≥1/week | 0.604*** (0.411, 0.798) | 0.615*** (0.325, 0.904) | 0.610*** (0.351, 0.869) | 0.407*** (0.257, 0.557) | 0.416*** (0.193, 0.639) | 0.413*** (0.211, 0.616) | 0.197*** (0.089, 0.306) | 0.199* (0.036, 0.361) | 0.197** (0.051, 0.343) |
| Interacting with friends (Ref: None) | |||||||||
| Not regularly | 0.097 (-0.144, 0.338) | 0.001 (-0.356, 0.356) | 0.175 (-0.151, 0.502) | 0.055 (-0.132, 0.242) | -0.018 (-0.292, 0.257) | 0.113 (-0.142, 0.368) | 0.042 (-0.093, 0.177) | 0.018 (-0.182, 0.218) | 0.063 (-0.120, 0.246) |
| ≥1/week | 0.518*** (0.324, 0.712) | 0.574*** (0.278, 0.870) | 0.490*** (0.232, 0.749) | 0.317*** (0.166, 0.468) | 0.386*** (0.158, 0.614) | 0.277** (0.075, 0.479) | 0.201*** (0.091, 0.310) | 0.188* (0.022, 0.354) | 0.214** (0.068, 0.359) |
| Mah-jong, cards, chess or other clubs (Ref: None) | |||||||||
| Not regularly | 0.240 (-0.078, 0.558) | 0.204 (-0.227, 0.635) | 0.299 (-0.172, 0.769) | 0.145 (-0.102, 0.392) | 0.113 (-0.219, 0.444) | 0.199 (-0.168, 0.567) | 0.095 (-0.084, 0.273) | 0.091 (-0.151, 0.333) | 0.099 (-0.165, 0.364) |
| ≥1/week | 0.640*** (0.326, 0.954) | 0.52* (0.086, 0.963) | 0.770*** (0.321, 1.219) | 0.589*** (0.345, 0.833) | 0.432* (0.094, 0.769) | 0.755*** (0.404, 1.106) | 0.051 (-0.126, 0.227) | 0.093 (-0.153, 0.339) | 0.015 (-0.238, 0.267) |
| Voluntary activities (Ref: None) | |||||||||
| Not regularly | 0.376** (0.121, 0.632) | 0.175 (-0.188, 0.538) | 0.557** (0.197, 0.917) | 0.230* (0.031, 0.428) | 0.096 (-0.184, 0.375) | 0.349* (0.068, 0.630) | 0.147* (0.003, 0.290) | 0.079 (-0.124, 0.283) | 0.209* (0.006, 0.411) |
| ≥1/week | 0.358+ (-0.054, 0.770) | 0.675* (0.071, 1.279) | 0.109 (-0.455, 0.673) | 0.154 (-0.166, 0.474) | 0.376 (-0.089, 0.841) | -0.018 (-0.459, 0.422) | 0.204+ (-0.027, 0.436) | 0.299+ (-0.040, 0.637) | 0.127 (-0.190, 0.444) |
| Sports or social clubs (Ref: No) | |||||||||
| Yes | 0.362* (0.042, 0.681) | 0.030 (-0.476, 0.537) | 0.530* (0.123, 0.938) | 0.161 (-0.087, 0.409) | 0.020 (-0.368, 0.409) | 0.229 (-0.090, 0.548) | 0.201* (0.022, 0.380) | 0.010 (-0.274, 0.294) | 0.301** (0.072, 0.531) |
| Internet (Ref: No) | |||||||||
| Yes | 0.644* (0.013, 1.273) | 0.731+ (-0.068, 1.530) | 0.549 (-0.470, 1.568) | 0.506* (0.017, 0.995) | 0.534+ (-0.081, 1.149) | 0.512 (-0.284, 1.308) | 0.138 (-0.216, 0.491) | 0.197 (-0.250, 0.645) | 0.037 (-0.536, 0.609) |
| Community organisations (Ref: No) | |||||||||
| Yes | 0.421 (-0.098, 0.939) | 0.159 (-0.572, 0.889) | 0.702+ (-0.033, 1.437) | 0.088 (-0.314, 0.491) | 0.036 (-0.526, 0.599) | 0.159 (-0.414, 0.734) | 0.333* (0.042, 0.624) | 0.122 (-0.287, 0.532) | 0.542** (0.130, 0.955) |
CI – confidence interval
*All models controlled time-varying variables, including year, education, marital status, living near children, retirement status, percapita household income, alcohol consumption, smoking, # of types of NCDs, and # of types of lower body constraints; + P < 0.1, * P < 0.05, ** P < 0.01, *** P < 0.001.
The association between SP and cognitive function varied across types of SP and between different dimensions of cognitive function ( Table 3 ). For interacting with friends and voluntary activities, taking part in these two types of SP was associated with an improved memory as well as mental status. Meanwhile, doing sports was only associated with improved mental status but not memory. On the contrary, for mah-jong and Internet use, a positive association was only observed in their relationship with memory but not mental status. No significant interaction effect with gender was found in any aspect of SP.
Using three waves of a longitudinal survey, this study examined the association between changes in SP and that in cognitive function among middle- and old-aged Chinese with the unobservable personal characteristics related variables controlled. This study has yielded four main findings: 1) a general downward trend was observed in all three dimensions of cognitive function with, however, improvement in memory function during 2011-2013; 2) the prevalence of SP varied across different types of SP, and an upward trend was observed in some activities; 3) more variety, higher frequency of SP was correlated with both better memory and mental status, whereas, the relationship varied across specific types of SP and between different dimensions of cognitive function; and 4) Gender-disparity was observed in the patterns of SP and cognitive function, but the association between SP and cognitive function remained similar in gender subgroups.
Changes of cognitive functions
In this study, we found that the cognitive function of middle- and old-aged respondents generally declined as they age. Supported by prior studies [ 25 , 26 ], this finding indicates that the threat of cognitive impairment may become more severe in the context of population ageing in China. Meanwhile, as we observed improvement in memory during 2011-2013, we noted that the trajectory was nonlinear, which is in line with some studies [ 10 , 11 ]. This finding reveals that it is still viable to improve one’s cognitive function with properly developed interventions even in their middle- and old-age. This reminds the value of identifying preventive approaches that would enable more people to enjoy their late-life with high quality [ 27 ].
Patterns of social participation
As a means with the potential to contribute to one’s cognitive function, the prevalence of SP was significantly lower in older Chinese compared with their counterparts in developed countries [ 20 ]. More interestingly, compared with western settings where community associations [ 28 ] and sport or social clubs [ 11 , 20 ] are more popular, mah-jong and interaction with friends were observed with higher prevalence amongst older Chinese. This echoes our proposition that cultural context should be taken into consideration when investigating the patterns of SP and its association with cognitive function. It is inspiring to observe a general uptrend of SP prevalence, such as diversity of SP and voluntary activities. This indicates that one’s social participation behaviour is intervene-able as long as the SP-friendly environment is well established.
Association between social participation and cognitive function
Consistent with our first hypothesis, this study found a significantly positive association between changes in diversity and frequency in SP and that in cognitive function. The finding is also in line with prior studies [ 19 , 29 ]. Moreover, we found that this relationship held across different dimensions of cognitive function and gender subgroups, which highlights the role of SP in predicting or even promoting cognitive function among middle- and old-aged Chinese [ 21 ].
Our results supported our second hypothesis that the strength of the association mainly depended on the type of activity and the dimension of cognitive function. We found that interacting with friends and voluntary activities were associated with better cognitive function in both memory and mental status; playing mah-jong and Internet use were only associated with better memory; whereas joining sports or social clubs was only associated with better mental status. A handful of prior studies have documented the type-related variations in this relationship [ 9 , 30 ], but few further investigated the relationship across different dimensions of cognitive function nor clarified the underlying mechanism.
With the underlying mechanism not fully comprehended, we speculate that different types of SP stimulate different parts of the brain with unique functions [ 31 ]. For instance, playing mah-jong requires attention and memory [ 32 ], and one’s fine motor movement and eye-hand coordination may be improved when playing mah-jong [ 33 ], which could contribute to enhancing brain function regarding digit forward and verbal memory [ 34 ]. This is similar for Internet use, which consists of novel and complex mental processes for older adults, especially requiring memory [ 15 ]. However, both mah-jong and Internet use tend to be indoor activities, whilst the part of the brain activated by them may not be closely related to time orientation or visuoconstruction. In contrast, sports tend to be outdoor activities in China. In other words, these types of activities may improve physiological functionality and stimulate the part of the brain that is associated with tasks involving time orientation, visuospatial [ 35 ], and mathematic performance [ 36 ]. Interacting with friends [ 16 ] and voluntary activities [ 37 ] were found to be associated with more extensive social networks and less depressive symptoms, which may contribute to better cognitive function via mitigating stress-related impact. Besides, the information exchange derived from inter-personal communication may help form healthy behaviours and have a more far-reaching influence on better cognitive performance [ 38 ]. As two types conventional SP in China, the identification of a significant association between cognitive function and mah-jong and interacting with friends suggested that policies to promote moderate mah-jong or interaction with friends may be worth consideration in light of its wide popularity [ 16 ]. Similarly, the growing prevalence of sports, such as square dance and Tai-chi [ 39 ], calls for special attention in policymaking.
Gender differences
Another interesting finding is the significant gender difference in the patterns of cognitive function and SP, but not in the relationship between these two. Women residents suffered from poor cognitive function and fewer chances for social activities when compared with their counterparts, which is consistent with prior studies [ 18 , 21 ]. This indicates that older women are in higher need for targeted SP to prevent cognitive impairment.
Prior findings regarding the gender-disparity in the relationship between SP and mental health are competing, as some reporting favourable effects only in women [ 40 ] or only in men [ 41 ], whereas some observed no gender differences [ 42 ]. The present study observed similar patterns in gender subgroups, and thus suggested that encouraging sufficient SP may be equally beneficial to men and women in China’s context. On the one hand, the finding echoes Tomioka et al. [ 19 ] who reminded the need to understand the relationship between SP and cognitive function in specific contexts. On the other hand, by acknowledging the complex mechanisms that underlie SP’s influence on cognitive function, this study calls for future studies to test whether there is a gender-difference in specific paths, such as through neurological health or mental health [ 43 ], with more sophisticated research design.
Strength and limitations
To the best of our knowledge, the present study is the first to examine the association between SP and cognitive function in China while ruling out the potential endogeneity that derives from personal characteristics such as gene and personality. Meanwhile, this study is one of the very few studies that further investigate the relationship in different dimensions of cognitive function and across different gender groups. These findings confirmed that more diversity and higher frequency of SP associated with better cognitive function in both men and women, suggested that conventional SP such as mah-jong or interacting with friends may be worth special attention, and also informed the type of SP that predicts improvements in the specific function of the brain in China’s context, which has implications for the development of targeted interventions.
The present study has several limitations. First, the study participants may not have fully represented the middle- and old-aged population in China, as the CHALS team conducted the survey among community-dwelling residents, whereas, those who live in institutions such as nursing home were not included. Second, information regarding participation in social activities was self-reported. The recall bias may result in underestimation of the SP behaviours due to hypomnesia in one’s older age. Third, this study assessed the contemptuous association between SP and cognitive function rather than the lagged effect, considering that SP brings contemporaneous effects to mental health that may diminish over time [ 20 ]. The causal relationship awaits further investigation. Fourth, the fixed-effects model has controlled individual-level time-invariant characteristics, nevertheless, there might be other unmeasurable or unmeasured time-varying variables not been included in this study. Fifth, the sample size for those who used Internet or joined community organisations were too small to be further categorised according to frequency. We delegate stratified analysis to future studies with a larger sample size.
Underpinned by a nationwide representative survey, we observed the patterns of SP behaviours and cognitive function in middle- and old-aged Chinese, and further explored the association between changes in SP and that in cognitive function by examining three dimensions of SP and two dimensions of cognitive function. The present study mainly revealed that: 1) more variety and higher frequency of of SP was generally associated with improved cognitive function, whereas the magnitude of the relationship depended on the specific type of SP and the dimension of cognitive functions; and 2) gender-disparity was observed in the patterns of SP and cognitive function, but the association between SP and cognitive function remained similar in gender subgroups.
.png)





